
Ch-6: Pharmacoeconomics (2 Hrs.)
Syllabus
Pharmacoeconomics – Introduction, basic terminologies, importance of Pharmacoeconomics
Introduction and Definition
- Pharmacoeconomics is the branch of health economics that evaluates the costs and outcomes of pharmaceutical products and services. It helps healthcare providers, governments, insurers, and pharmaceutical companies decide which medicines provide the best value for money.
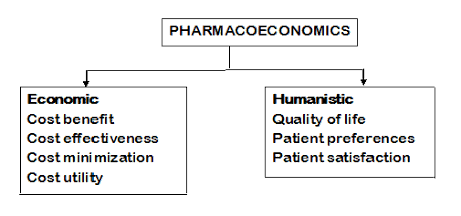
- Pharmacoeconomics can also be defined as , “branch of economics that uses cost-benefit, cost-effectiveness, cost-minimisation, cost-of-illness and cost utility analysis to compare pharmaceutical products and treatment strategies”
- Its primary goal isn’t simply to find the cheapest drug, but to determine which therapy provides the maximum therapeutic benefit for the lowest possible cost. This data is critical for formulary development, pricing negotiations, and ensuring the optimal allocation of limited healthcare resources.
Methods of Pharmacoeconomics evaluation
There are four methods of Pharmacoeconomics evaluation:
- Cost-Minimization Analysis (CMA)
- Cost-Effectiveness Analysis (CEA)
- Cost-Utility Analysis (CUA)
- Cost-Benefit Analysis (CBA)
1. Cost-Minimization Analysis (CMA)
- Cost-Minimization Analysis (CMA) is the most basic form of pharmacoeconomic evaluation. It is used to compare the total costs of two or more alternative therapies that have already been proven to have identical clinical efficacy and safety profiles.
- To find the least expensive option among therapies proven to have the exact same clinical efficacy (e.g., brand vs. generic).
- The absolute prerequisite for using CMA is proven clinical equivalence. You cannot use this method if one drug works slightly faster, has fewer side effects, or results in a better quality of life than the other. If the outcomes differ in any way, you must use a Cost-Effectiveness Analysis (CEA) or Cost-Utility Analysis (CUA) instead.
- When is CMA Used in Pharmacy?
- Brand vs. Generic Equivalents: Comparing a branded medication (e.g., Lipitor) to its generic counterpart (atorvastatin). Since the active ingredient, dose, and bioavailability are identical, the decision is purely financial.
- Different Routes of Administration: Comparing the total cost of administering the same drug intravenously (IV) versus orally, assuming the clinical outcome for the patient’s specific condition is proven equal.
- Different Treatment Settings: Evaluating the cost of receiving the same IV antibiotic therapy in a hospital setting versus via home healthcare.
- Different Dosing Regimens: Comparing a once-daily extended-release formulation to a three-times-daily immediate-release formulation of the exact same drug, provided they achieve identical therapeutic goals.
2. Cost-Effectiveness Analysis (CEA)
- Cost-Effectiveness Analysis (CEA) is the most widely used and comprehensive pharmacoeconomic evaluation method. While Cost-Minimization Analysis (CMA) assumes two drugs are identical, Cost-Effectiveness Analysis (CEA) is used to compare treatments that have the same clinical objective but different levels of efficacy and cost.
- The goal is to determine if the added clinical benefit of a newer, more effective drug mathematically justifies its higher price tag.
- To compare therapies with different efficacy levels but the same clinical objective.
3. Cost-Utility Analysis (CUA)
- When a treatment significantly impacts the quality of life, not just biological markers (e.g., chemotherapy).
- Cost-Utility Analysis (CUA) is the most sophisticated form of pharmacoeconomic evaluation. Like Cost-Effectiveness Analysis (CEA), it compares the costs and clinical outcomes of different treatments.
- However, CUA solves a major limitation of CEA: it accounts for how a patient actually feels. Instead of measuring outcomes in natural units (like blood pressure or cholesterol levels), CUA measures outcomes using a specialized metric that combines both the quantity (length) and quality of life.
4. Cost-Benefit Analysis (CBA)
- Cost-Benefit Analysis (CBA) is a pharmacoeconomic method where both the costs of a healthcare intervention and its health outcomes (benefits) are measured in the exact same unit: money.
- Cost-Benefit Analysis (CBA) can also be defined as is a pharmacoeconomic method in which both the costs and benefits of a healthcare intervention are measured in monetary terms.
- Unlike the other three evaluation methods (CMA, CEA, and CUA) which measure outcomes in clinical units or QALYs (Quality adjusted life years), CBA assigns a strict financial value to everything—including symptom relief, avoided hospitalizations, and even human life itself.
- To compare interventions across entirely different healthcare sectors (e.g., a vaccination program vs. buying an MRI machine).
- It is used to determine whether the benefits of a treatment or program outweigh its costs.
Importance of Pharmacoeconomics
Pharmacoeconomics is important because it helps ensure the best use of limited healthcare resources by comparing the cost and outcomes of drug therapies and healthcare services.
Major Importance of Pharmacoeconomics
- Promotes Rational Use of Medicines
- Reduces Healthcare Costs
- Improves Patient Care
- Assists Healthcare Policy Decisions
- Supports Drug Pricing and Reimbursement
- Helps Pharmaceutical Industries
- Aids Clinical Decision-Making
- Enhances Resource Allocation
Simple One-Line Definition
“Pharmacoeconomics is important because it helps achieve maximum healthcare benefit at minimum cost.”
Stake holders of Pharmacoeconomics
A health intervention that looks highly attractive from one point of view might look entirely unfeasible from another. To understand how pharmacoeconomic decisions are made, you must understand the perspectives of the four primary stakeholders.
- The Pharmaceutical Industry/ Manufacturers
- Health care practitioners/prescribers
- Pharmacist
- Patients
1. The Pharmaceutical Industry (Manufacturers)
- Pharmaceutical companies invest billions in Research and Development (R&D). They need to prove their innovations hold economic value to successfully sell them.
- Primary Perspective: Return on investment, market access, and pricing justification.
- Key Focus Areas: Highlighting long-term cost offsets. A manufacturer might argue that while their new drug has a high acquisition cost, it prevents expensive hospitalizations later on (saving the payer money in the long run).
- How They Benefit: Robust pharmacoeconomic modelling is used to negotiate market entry prices with government health ministries and secure favourable placement on insurance formularies.
- The pharmaceutical industry occupies a unique position in the pharmacoeconomic landscape. Unlike patients, who are primarily concerned with consuming or funding healthcare, the pharmaceutical industry is the innovator and supplier.
- For manufacturers, Pharmacoeconomics is not just an academic exercise; it is a critical business tool known as Health Economics and Outcomes Research (HEOR). It dictates whether a drug is developed, how much it will cost, and whether it will ultimately succeed in the market.
- Here is a detailed breakdown of how the pharmaceutical industry utilizes Pharmacoeconomics as a key stakeholder:
- Guiding Research and Development (R&D) Decisions: The journey of bringing a single new drug to market can take over a decade and cost billions of dollars. Manufacturers use early pharmacoeconomic modeling to decide which drugs in their pipeline are worth pursuing.
- Pricing Strategy and Justification: Once a drug is proven safe and effective, the manufacturer must set a price. They cannot simply pick a number; they must mathematically justify the price tag to government health ministries and private insurers.
- Value-Based Pricing: Instead of pricing a drug based on what it cost to manufacture, companies price it based on the economic value it brings to the healthcare system.
- Highlighting Cost Offsets: A manufacturer will use Cost-Benefit Analysis (CBA) or Cost-Effectiveness Analysis (CEA) to argue that while their drug has a high acquisition cost, it prevents expensive events down the line. For example, a company selling a very expensive heart failure medication will use data to prove that the drug significantly reduces the need for ICU admissions, ultimately saving the health system money.
- The Manufacturer’s Ultimate Goal: By proving their products provide measurable economic value, they secure market access, formulary placement, and a return on their R&D investment.
2. Health care practitioners/prescribers
- Here is the simplest way to understand the role of healthcare practitioners (like doctors and prescribers) in pharmacoeconomics, structured cleanly for quick reference or study notes:
- Think of the prescriber as the navigator for the patient’s health journey.
- While the government worries about the national budget, the prescriber is standing right in front of the patient. Their job is to map out the best route to get the patient healthy, while making sure the “ticket” isn’t so expensive that the patient refuses to take the trip.
- Here is how they use pharmacoeconomics in real life:
- Safety First, Price Second: Their number one legal and ethical job is to cure the patient. They only start thinking about costs after they have narrowed down the list of drugs to the ones that are proven safe and effective for that specific disease.
- The “Reality Check” (Preventing Non-Adherence): A perfect prescription on paper is completely useless if the patient leaves it at the pharmacy counter because it costs too much. Prescribers use pharmacoeconomics to match the treatment to the patient’s wallet. If they know a patient is on a tight budget, they will intentionally prescribe a cheaper, older drug that still works well, rather than a brand-new, expensive one that the patient will just stop taking.
- To the prescriber, pharmacoeconomics is about being a practical healer. They use economic thinking to ensure the cost of the medicine doesn’t create a new burden for the patient they are trying to cure.
3. Pharmacist
- Think of the pharmacist as the financial guardian of patient care. While pharmaceutical companies set the prices and insurance companies set the budgets, the pharmacist is the one standing at the pharmacy counter or on the hospital floor, making sure the math actually works for the patient.
- Here is a clear, simplified breakdown of how pharmacists act as key players in pharmacoeconomics—structured perfectly for easy reading or study notes:
- The Master of Generic Substitution (Cost-Minimization): When a doctor writes a prescription for a very expensive brand-name drug, the pharmacist steps in to find the equivalent. The patient gets the exact same clinical benefit (identical active ingredient) but saves a significant amount of money. This is the most common real-world application of Cost-Minimization Analysis (CMA).
- The IV-to-Oral Switcher: In a hospital setting, intravenous (IV) drugs are incredibly expensive. The cost includes not just the drug, but the IV bags, the tubing, and the nursing time required to administer and monitor it.
- As soon as a patient’s digestive system is working and they are stable, the clinical pharmacist recommends switching them from an IV drip to a simple oral pill.
- Pharmacists are the practical economists of the healthcare system. They use their deep clinical expertise to ensure that every rupee spent on medication delivers the maximum possible health benefit to the patient.
4. Patients
- Think of the patient as the person buying a pair of shoes someone else picked out.
- The doctor chooses the shoe (the prescription), and the insurance company helps pay for part of it, but the patient is the one who actually has to walk in them every day.
- Here is how the patient looks at pharmacoeconomics in the real world:
- The Price Tag (Out-of-Pocket Cost): Patients don’t care if a drug cost a billion dollars to invent in a lab. They only care about the final price the pharmacist asks them to pay. If that amount to be paid is higher than what they have in their bank account, they leave the medicine on the counter.
- The Hidden Hassles (Indirect Costs): It’s not just about the price of the pill. If getting a treatment means missing a day of work, paying for a babysitter, and sitting in hospital traffic, the patient is paying with their lost wages and time. A “cheap” IV drug is actually very expensive for a patient if it costs them their daily income to go to the clinic.
- The Bottom Line: To a patient, a drug is only “cost-effective” if they can comfortably afford to buy it, have the time to take it, and can tolerate how it makes them feel.